The end of closed reduction
Closed reposition, i.e. the setting of the dislocated hip joint (insertion of the femoral head into the acetabulum) under general anesthesia (along with muscle tension paralysis, it allows the femoral head to be inserted if the cause are contracted muscles and a non-cooperating infant.
Unfortunately, nature does not tolerate vacuum and if it lasts too long for more than 10 days: the empty cup is filled with soft tissues and an overgrown elongated femoral ligament / which prevent the correct spontaneous positioning of the head. Nevertheless, it stabilizes in this position with a plaster.
100% of blood circulation disorders and necrosis occurs after the end of anesthesia, muscle tension and contractures return more than before anesthesia in the new position The child cries without interruption due to ischemia up to 3 days when the nerve endings died .and the head stops rebuilding until the blood vessels are rebuilt, which lasts up to 3 months 1mm a day
in this case the plaster should be pulled off immediately
At the age of 6m, the bone acetabulum should be rebuilt within mx weeks, this is how much the fractures heal, if it lasts longer, it indicates the occurrence of ischemia and lack of blood supply to the bones as in other bone reconstructions in fractures, etc.
These treatments remained from the times when the rehabilitation of infants was underdeveloped. Nowadays, there are great developed and specialized teams for the rehabilitation of newborns and infants, removing such fresh temporary contractures is not a problem for them.
Time to rethink the use of hip spica cast, over head or anesthesia to stretch the contracted muscles due to displacement of the femoral head in Ddh.Caused by non-elevated muscle tension or permanent damage to the muscular nervous system,
these changes are short-lived and last a few months due to mechanical displacement.
Rehabilitators dealing with infants with muscle contractures in PCI easily remove them .
. If 3 x 20 minutes every other day is enough to remove muscle contracture in infants, the more strains can also be removed, they only require more work.
The head of the femur lies superficially and is accessible for rehabilitation as well as the surrounding muscles.
The use of multiple days without breaks in the procedure causes only blood circulation disorders and necrosis (avn).
Patient and tedious rehabilitation with a non-cooperating infant is enough to improve. Muscle cramps recur as the child grows, so the exercises need to be repeated from time to time.
The problem is that ligaments are stronger than the bones in this age and it is easier to damage the bones and the easiest way to disturb the blood supply is that the vessels close
before the end of the maximum muscle tone, the main artery which scrolls around the m. lipsoas.
stretching it is the most problematic because there is no access to it almost completely because it is inside the body.
case Natalii
typ IV right hip diagnosis 1month; tratment with orthesis wthout effect for 5 months
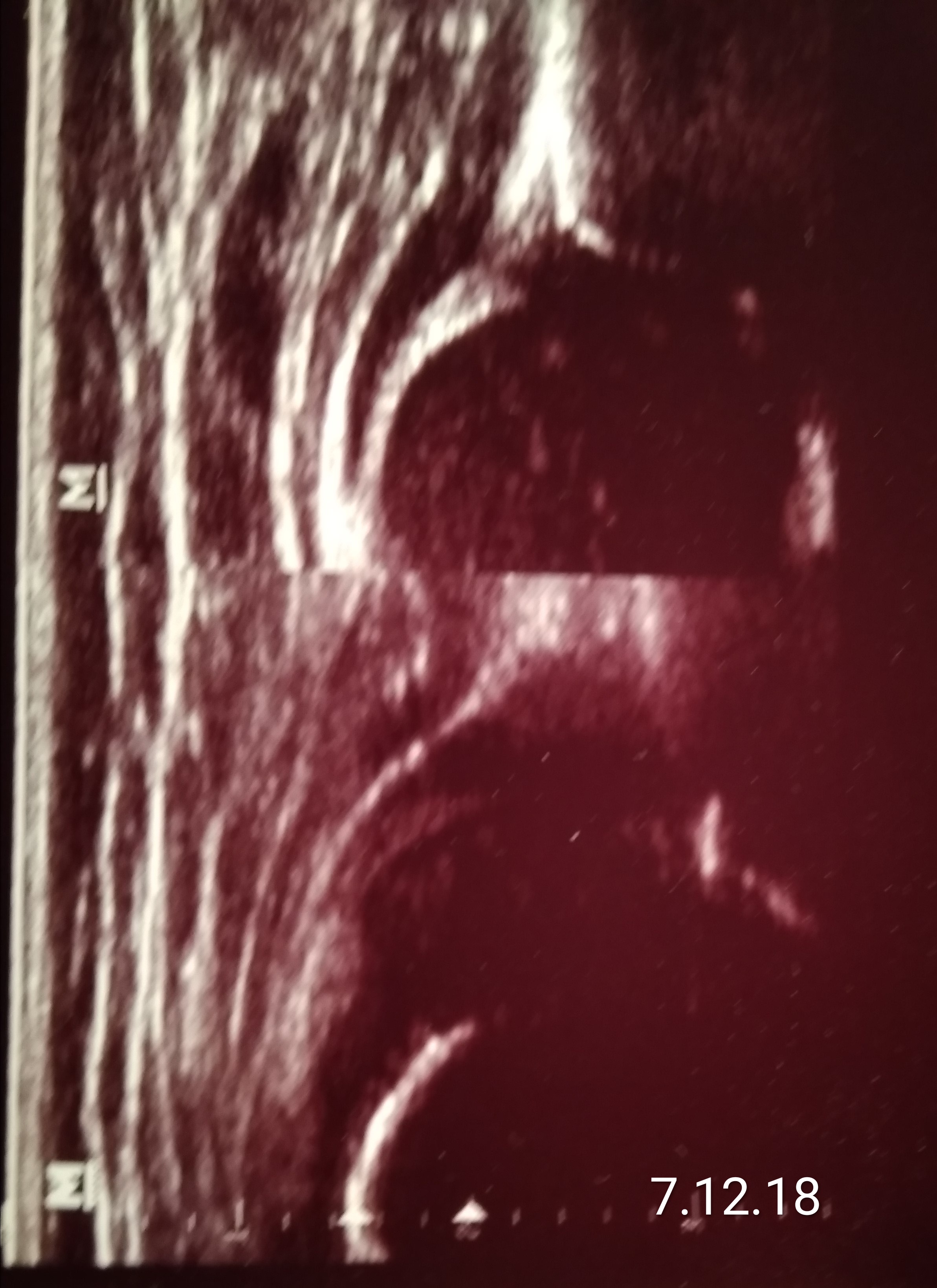
rehabilitation was ordered ;
slowy increase from 3 time a week to 3 time a day ( 20 minutes each time)
type IIb but unfortunataly unstable becouse with overgrown lig. capitis fem. (big white echo on the right and below side of the femur's head )
